Abstract
Mature teratomas are the third most common mediastinal tumors. Giant teratoma in pediatric population is rare. A resection of giant benign teratoma in left hemithorax was performed in a 4-year-old patient. The computed tomography scan showed the presence of a large multiloculated mediastinal mass extending to the left pleural space and pleural effusion. The patient underwent total resection of the mediastinal mass via a median sternotomy associated to left anterior thoracotomy. Entry into the pleural space was performed through the sixth intercostal space to obtain safe visualization of the cavity and proceed to tumor excision. The collapsed left lung was re-expanded, and the patient was extubated. Despite the size and the surrounding structures of the teratoma, our preoperative preparation and surgical technique were effective and resulted in favorable recovery without complications and a posterior normal left lung function.Δευτέρα 14 Σεπτεμβρίου 2020
Giant benign teratoma occupying the left hemithorax with pleural effusion: a rare presentation
Giant benign teratoma occupying the left hemithorax with pleural effusion: a rare presentation:
Benign cyst with xanthogranulomatous inflammation involving the transverse colon and the common iliac artery
Benign cyst with xanthogranulomatous inflammation involving the transverse colon and the common iliac artery:
Abstract
Xanthogranulomatous inflammation (XGI) is a rare process. Colonic XGI is extremely rare. We present a case report of XGI arising within an intra-abdominal cyst involving the transverse colon. A 28-year-old man presented with abdominal discomfort. He underwent a computed tomography abdomen–pelvis, which found three subcutaneous collections and a large cystic intra-abdominal structure. The decision was made for resection. Intraoperatively, the cyst originated from the pelvis and was adherent to the surrounding tissues. Histology from the lesion revealed XGI extending into the surrounding tissue. XGI is a rare inflammatory condition. Clinically, it can be difficult to distinguish XGI from an infiltrative malignancy. Therefore, it is usually necessary to obtain a pathological diagnosis of XGI. This case describes an atypical cystic lesion with XGI involving the transverse colon. Although rare, it should be considered in the potential differential diagnosis of an infective or malignant mesenteric cyst.Extended right posterior liver sectionectomy for HCC in a patient with left ventricular assist device—a case report
Extended right posterior liver sectionectomy for HCC in a patient with left ventricular assist device—a case report:
Abstract
Successful implementation of left ventricular assist devices lead to a prolonged survival in patients with chronic terminal heart failure. Thus, patients with pre-existing left ventricular assist devices with abdominal comorbidities requiring abdominal surgery, e.g. for malignancy, are upcoming issues. We carried out a major liver resection for hepatocellular carcinoma in a patient with pre-existing left ventricular assist device. The importance of this case report is that it outlines the significance of oncologic resections in patients with left ventricular assist devices as an upcoming issue and provides an interdisciplinary approach.Emergency surgery for acute cholecystitis associated with cholecystocolonic fistula caused by gallbladder cancer
03:00
by Sunakawa T, Ko K, Moriyasu R, et al. via  Journal of Surgical Case Reports - current issue
Journal of Surgical Case Reports - current issue
Abstract
Preoperative diagnosis of cholecystocolonic fistula (CCF) is difficult and the contribution of gallbladder cancer or colon cancer is unclear when there is associated malignancy. We present a case that was diagnosed with acute cholecystitis associated with CCF by multidetector computed tomography (MDCT) preoperatively and malignant neoplasm during emergency surgery. She was finally diagnosed with gallbladder cancer after the operation and underwent a two-stage surgery for regional lymph node dissection. Gallbladder cancer can be a primary malignant cancer causing CCF, whereas MDCT is useful for preoperative diagnosis of CCF. A treatment plan in consideration of gallbladder cancer is advisable for CCF associated with malignant tumor.inoperable or recurrent HER2-positive breast cancer: similar efficacy and safety for pertuzumab plus trastuzumab and docetaxel
The efficacy and safety of pertuzumab plus trastuzumab and docetaxel as a first-line therapy in Japanese patients with inoperable or recurrent HER2-positive breast cancer: the COMACHI study.:
The efficacy and safety of pertuzumab plus trastuzumab and docetaxel as a first-line therapy in Japanese patients with inoperable or recurrent HER2-positive breast cancer: the COMACHI study.
Breast Cancer Res Treat. 2020 Sep 13;:
Authors: Takahashi M, Ohtani S, Nagai SE, Takashima S, Yamaguchi M, Tsuneizumi M, Komoike Y, Osako T, Ito Y, Ikeda M, Ishida K, Nakayama T, Takashima T, Asakawa T, Matsumoto S, Shimizu D, Masuda N
Abstract
PURPOSE: In the CLEOPATRA study of patients with human epidermal growth factor receptor 2 (HER2)-positive recurrent or metastatic breast cancer, the Japanese patient subgroup did not demonstrate the improved progression-free survival (PFS) of pertuzumab plus trastuzumab and docetaxel vs. placebo that was seen in the overall population. Therefore, COMACHI was conducted to confirm the efficacy and safety of this treatment regimen in this patient subgroup.
METHODS: This was a phase IV study of pertuzumab plus trastuzumab and docetaxel in Japanese patients with histologically/cytologically confirmed inoperable or recurrent HER2-positive breast cancer. All patients received pertuzumab, trastuzumab, and docetaxel intravenously every 3 weeks until disease progression/unacceptable toxicity. The primary endpoint was investigator-assessed PFS. Secondary endpoints were overall survival (OS), investigator-assessed objective response rate, and duration of response (DoR). Safety was also assessed.
RESULTS: At final analysis, median investigator-assessed PFS was 22.8 months (95% CI 16.9-37.5). From first dose, OS rate at 1 year was 97.7%; and at 2 and 3 years were 88.5% and 79.1%, respectively. Of the 118 patients with measurable disease at baseline, response rate was 83.9% (95% CI 77.3-90.5) and median investigator-assessed DoR was 26.3 months (95% CI 17.1-not evaluable). Treatment was well tolerated, with no new safety signals detected.
CONCLUSIONS: Our results suggest similar efficacy and safety for pertuzumab plus trastuzumab and docetaxel in Japanese patients compared with the overall population of CLEOPATRA, providing further support for this combination therapy as standard of care for Japanese patients with inoperable or recurrent HER2-positive breast cancer.
PMID: 32920732 [PubMed - as supplied by publisher]
Breast Cancer Res Treat. 2020 Sep 13;:
Authors: Takahashi M, Ohtani S, Nagai SE, Takashima S, Yamaguchi M, Tsuneizumi M, Komoike Y, Osako T, Ito Y, Ikeda M, Ishida K, Nakayama T, Takashima T, Asakawa T, Matsumoto S, Shimizu D, Masuda N
Abstract
PURPOSE: In the CLEOPATRA study of patients with human epidermal growth factor receptor 2 (HER2)-positive recurrent or metastatic breast cancer, the Japanese patient subgroup did not demonstrate the improved progression-free survival (PFS) of pertuzumab plus trastuzumab and docetaxel vs. placebo that was seen in the overall population. Therefore, COMACHI was conducted to confirm the efficacy and safety of this treatment regimen in this patient subgroup.
METHODS: This was a phase IV study of pertuzumab plus trastuzumab and docetaxel in Japanese patients with histologically/cytologically confirmed inoperable or recurrent HER2-positive breast cancer. All patients received pertuzumab, trastuzumab, and docetaxel intravenously every 3 weeks until disease progression/unacceptable toxicity. The primary endpoint was investigator-assessed PFS. Secondary endpoints were overall survival (OS), investigator-assessed objective response rate, and duration of response (DoR). Safety was also assessed.
RESULTS: At final analysis, median investigator-assessed PFS was 22.8 months (95% CI 16.9-37.5). From first dose, OS rate at 1 year was 97.7%; and at 2 and 3 years were 88.5% and 79.1%, respectively. Of the 118 patients with measurable disease at baseline, response rate was 83.9% (95% CI 77.3-90.5) and median investigator-assessed DoR was 26.3 months (95% CI 17.1-not evaluable). Treatment was well tolerated, with no new safety signals detected.
CONCLUSIONS: Our results suggest similar efficacy and safety for pertuzumab plus trastuzumab and docetaxel in Japanese patients compared with the overall population of CLEOPATRA, providing further support for this combination therapy as standard of care for Japanese patients with inoperable or recurrent HER2-positive breast cancer.
PMID: 32920732 [PubMed - as supplied by publisher]
Serum cystatin C: A potential predictor for hospital-acquired acute kidney injury in patients with acute exacerbation of COPD
Serum cystatin C: A potential predictor for hospital-acquired acute kidney injury in patients with acute exacerbation of COPD: Chronic Respiratory Disease, Volume 17, Issue , January-December 2020.
Hospital-acquired acute kidney injury (HA-AKI) is associated with poor prognosis. In this study, we evaluated whether serum cystatin C on admission could predict AKI in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD). The retrospective study was conducted using data on adult inpatients with AECOPD from January 2014 to January 2017. A total of 1035 patients were included, among which 79 (7.6%) with HA-AKI were identified. Univariate and multivariate logistic regression analyses were used to investigate predictors of HA-AKI in patients with AECOPD. HA-AKI was associated with poor prognosis, and patients with HA-AKI had higher inpatient mortality (34.2% vs. 2.6%, p < 0.001). Furthermore, after adjusting for confounders, HA-AKI was an independent risk factor for inpatient mortality for patients with AECOPD (odds ratio (OR) 11.02; 95% confidence interval (CI) 4.77–25.45; p < 0.001). Four independent risk factors for HA-AKI (age, levels of urea and cystatin C, and platelet count on admission) were identified in patients with AECOPD. Cystatin C (OR 5.22; 95% CI 2.49–10.95; p < 0.001) was a significant independent predictor of AKI in patients with AECOPD. HA-AKI in patients with AECOPD could be identified with a sensitivity of 73.5% and a specificity of 75.9% (area under the curve (AUC) = 0.803, 95% CI 0.747–0.859) by cystatin C level (cutoff value = 1.3 mg/L) and with a sensitivity of 75.9% and a specificity of 82.0% (AUC = 0.853, 95% CI 0.810–0.896) using a model comprising all significant predictors. Serum cystatin C has the potential for use to predict the risk of HA-AKI in patients with AECOPD.
Hospital-acquired acute kidney injury (HA-AKI) is associated with poor prognosis. In this study, we evaluated whether serum cystatin C on admission could predict AKI in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD). The retrospective study was conducted using data on adult inpatients with AECOPD from January 2014 to January 2017. A total of 1035 patients were included, among which 79 (7.6%) with HA-AKI were identified. Univariate and multivariate logistic regression analyses were used to investigate predictors of HA-AKI in patients with AECOPD. HA-AKI was associated with poor prognosis, and patients with HA-AKI had higher inpatient mortality (34.2% vs. 2.6%, p < 0.001). Furthermore, after adjusting for confounders, HA-AKI was an independent risk factor for inpatient mortality for patients with AECOPD (odds ratio (OR) 11.02; 95% confidence interval (CI) 4.77–25.45; p < 0.001). Four independent risk factors for HA-AKI (age, levels of urea and cystatin C, and platelet count on admission) were identified in patients with AECOPD. Cystatin C (OR 5.22; 95% CI 2.49–10.95; p < 0.001) was a significant independent predictor of AKI in patients with AECOPD. HA-AKI in patients with AECOPD could be identified with a sensitivity of 73.5% and a specificity of 75.9% (area under the curve (AUC) = 0.803, 95% CI 0.747–0.859) by cystatin C level (cutoff value = 1.3 mg/L) and with a sensitivity of 75.9% and a specificity of 82.0% (AUC = 0.853, 95% CI 0.810–0.896) using a model comprising all significant predictors. Serum cystatin C has the potential for use to predict the risk of HA-AKI in patients with AECOPD.
Management Strategies of Ocular Chemical Burns: Current Perspectives
Management Strategies of Ocular Chemical Burns: Current Perspectives:
Abstract: Ocular chemical burns are absolute ophthalmic emergencies and require immediate management to minimize devastating sequelae. Management of alkali and acid burns is started at the scene of the accident by copious irrigation. Treatment is directed at improving epithelial integrity and stromal stability, reduction of undue inflammation, and prevention or timely management of complications. To ascertain the best possible outcome, numerous biological medications and surgical interventions have been merged into conventional therapeutic regimens. These include autologous and umbilical cord serum preparations, platelet-rich plasma, amniotic membrane transplantation, limbal stem-cell transplantation, and anti-angiogenic agents.
Keywords: ocular chemical burn, amniotic membrane transplantation, autologous serum, limbal stem cell transplantation
Abstract: Ocular chemical burns are absolute ophthalmic emergencies and require immediate management to minimize devastating sequelae. Management of alkali and acid burns is started at the scene of the accident by copious irrigation. Treatment is directed at improving epithelial integrity and stromal stability, reduction of undue inflammation, and prevention or timely management of complications. To ascertain the best possible outcome, numerous biological medications and surgical interventions have been merged into conventional therapeutic regimens. These include autologous and umbilical cord serum preparations, platelet-rich plasma, amniotic membrane transplantation, limbal stem-cell transplantation, and anti-angiogenic agents.
Keywords: ocular chemical burn, amniotic membrane transplantation, autologous serum, limbal stem cell transplantation
A Real-World Study of Dexamethasone Implant in Treatment-Naïve Patients with Diabetic Macular Edema: Efficacy and Correlation Between Inflammatory Biomarkers and Treatment Outcome
A Real-World Study of Dexamethasone Implant in Treatment-Naïve Patients with Diabetic Macular Edema: Efficacy and Correlation Between Inflammatory Biomarkers and Treatment Outcome:
Purpose: There has been an increasing clinical interest in specific retinal parameters as non-invasive biomarkers of retinal inflammation in diabetic macular edema (DME) that have been shown to have prognostic value, such as hyperreflective retinal fields (HRFs) and subfoveal neuroretinal detachment (SND).
Methods: We conducted a prospective, non-comparative study of treatment-naïve patients with DME to evaluate the efficacy of a Pro Re Nata (PRN) regimen of intravitreal dexamethasone implant 0.7 mg (DexI, Ozurdex™). After administration, patients underwent subsequent injections according to PRN criteria in case of edema relapse, but not earlier than 4 months after the previous treatment. Patients were evaluated at baseline, within 15 days of injection, and every month thereafter. During all visits, best-corrected visual acuity (BCVA) was recorded; central retinal thickness (CRT), type of edema, presence of SND, and presence and number of HRFs were evaluated using swept-source optical coherence tomography (SS-OCT) 3D. Treatment outcome was defined as changes in BCVA, CRT, SND and HRFs at 12 (T12) and 24 (T24) months compared with baseline (T0).
Results: The study enrolled 24 eyes of 18 patients. The mean duration of follow-up was 18± 6.6 months; for all eyes, T12 data were available, while follow-up reached T24 for 12 eyes. BCVA improved significantly and CRT decreased significantly during treatment; the edema was no longer detectable in 13/24 eyes at T12 and 8/12 eyes at T24. No patient presented SND at T12 and T24, and the mean number of HRFs decreased significantly during treatment. Results with CRT and HRFs correlated with BCVA at 12 and 24 months. No significant adverse events were observed.
Conclusion: In patients with DME, the intravitreal dexamethasone implant was effective and safe in improving both functional and tomographic parameters. This result is consistent with improvement in biomarkers of inflammation.
Keywords: dexamethasone implant, diabetic macular edema, intravitreal implants, Ozurdex, real-world, inflammation
Purpose: There has been an increasing clinical interest in specific retinal parameters as non-invasive biomarkers of retinal inflammation in diabetic macular edema (DME) that have been shown to have prognostic value, such as hyperreflective retinal fields (HRFs) and subfoveal neuroretinal detachment (SND).
Methods: We conducted a prospective, non-comparative study of treatment-naïve patients with DME to evaluate the efficacy of a Pro Re Nata (PRN) regimen of intravitreal dexamethasone implant 0.7 mg (DexI, Ozurdex™). After administration, patients underwent subsequent injections according to PRN criteria in case of edema relapse, but not earlier than 4 months after the previous treatment. Patients were evaluated at baseline, within 15 days of injection, and every month thereafter. During all visits, best-corrected visual acuity (BCVA) was recorded; central retinal thickness (CRT), type of edema, presence of SND, and presence and number of HRFs were evaluated using swept-source optical coherence tomography (SS-OCT) 3D. Treatment outcome was defined as changes in BCVA, CRT, SND and HRFs at 12 (T12) and 24 (T24) months compared with baseline (T0).
Results: The study enrolled 24 eyes of 18 patients. The mean duration of follow-up was 18± 6.6 months; for all eyes, T12 data were available, while follow-up reached T24 for 12 eyes. BCVA improved significantly and CRT decreased significantly during treatment; the edema was no longer detectable in 13/24 eyes at T12 and 8/12 eyes at T24. No patient presented SND at T12 and T24, and the mean number of HRFs decreased significantly during treatment. Results with CRT and HRFs correlated with BCVA at 12 and 24 months. No significant adverse events were observed.
Conclusion: In patients with DME, the intravitreal dexamethasone implant was effective and safe in improving both functional and tomographic parameters. This result is consistent with improvement in biomarkers of inflammation.
Keywords: dexamethasone implant, diabetic macular edema, intravitreal implants, Ozurdex, real-world, inflammation
Collagen-Supplemented Incubation Rapidly Augments Mechanical Property of Fibroblast Cell Sheets
Collagen-Supplemented Incubation Rapidly Augments Mechanical Property of Fibroblast Cell Sheets: Tissue Engineering Part A, Ahead of Print.Abstract
Cell sheet technology using UpCell™ (Thermo Fisher Scientific, Roskilde, Denmark) plates is a modern tool that enables the rapid creation of single-layered cells without using extracellular matrix (ECM) enzymatic digestion. Although this technique has the advantage of maintaining a sheet of cells without needing artificial scaffolds, these cell sheets remain extremely fragile. Collagen, the most abundant ECM component, is an attractive candidate for modulating tissue mechanical properties given its tunable property. In this study, we demonstrated rapid mechanical property augmentation of human dermal fibroblast cell sheets after incubation with bovine type I collagen for 24 h on UpCell plates. We showed that treatment with collagen resulted in increased collagen I incorporation within the cell sheet without affecting cell morphology, cell type, or cell sheet quality. Atomic force microscopy measurements for controls, and cell sheets that received 50 and 100 μg/mL collagen I treatments revealed an average Young's modulus of their respective intercellular regions: 6.6 ± 1.0, 14.4 ± 6.6, and 19.8 ± 3.8 kPa during the loading condition, and 10.3 ± 4.7, 11.7 ± 2.2, and 18.1 ± 3.4 kPa during the unloading condition. This methodology of rapid mechanical property augmentation of a cell sheet has a potential impact on cell sheet technology by improving the ease of construct manipulation, enabling new translational tissue engineering applications.
Cell sheet technology using UpCell™ (Thermo Fisher Scientific, Roskilde, Denmark) plates is a modern tool that enables the rapid creation of single-layered cells without using extracellular matrix (ECM) enzymatic digestion. Although this technique has the advantage of maintaining a sheet of cells without needing artificial scaffolds, these cell sheets remain extremely fragile. Collagen, the most abundant ECM component, is an attractive candidate for modulating tissue mechanical properties given its tunable property. In this study, we demonstrated rapid mechanical property augmentation of human dermal fibroblast cell sheets after incubation with bovine type I collagen for 24 h on UpCell plates. We showed that treatment with collagen resulted in increased collagen I incorporation within the cell sheet without affecting cell morphology, cell type, or cell sheet quality. Atomic force microscopy measurements for controls, and cell sheets that received 50 and 100 μg/mL collagen I treatments revealed an average Young's modulus of their respective intercellular regions: 6.6 ± 1.0, 14.4 ± 6.6, and 19.8 ± 3.8 kPa during the loading condition, and 10.3 ± 4.7, 11.7 ± 2.2, and 18.1 ± 3.4 kPa during the unloading condition. This methodology of rapid mechanical property augmentation of a cell sheet has a potential impact on cell sheet technology by improving the ease of construct manipulation, enabling new translational tissue engineering applications.
The effect of vitamin D supplementation on survival in patients with colorectal cancer: systematic review and meta-analysis of randomised controlled trials
The effect of vitamin D supplementation on survival in patients with colorectal cancer: systematic review and meta-analysis of randomised controlled trials:
British Journal of Cancer, Published online: 15 September 2020; doi:10.1038/s41416-020-01060-8
The effect of vitamin D supplementation on survival in patients with colorectal cancer: systematic review and meta-analysis of randomised controlled trials
Abstract
Background
Low circulating vitamin D levels are associated with poor colorectal cancer (CRC) survival. We assess whether vitamin D supplementation improves CRC survival outcomes.
Methods
PubMed and Web of Science were searched. Randomised controlled trial (RCTs) of vitamin D supplementation reporting CRC mortality were included. RCTs with high risk of bias were excluded from analysis. Random-effects meta-analysis models calculated estimates of survival benefit with supplementation. The review is registered on PROSPERO, registration number: CRD42020173397.
Results
Seven RCTs (n = 957 CRC cases) were identified: three trials included patients with CRC at outset, and four population trials reported survival in incident cases. Two RCTs were excluded from meta-analysis (high risk of bias; no hazard ratio (HR)). While trials varied in inclusion criteria, intervention dose and outcomes, meta-analysis found a 30% reduction in adverse CRC outcomes with supplementation (n = 815, HR = 0.70; 95% confidence interval (CI): 0.48–0.93). A beneficial effect was seen in trials of CRC patients (progression-free survival, HR = 0.65; 95% CI: 0.36–0.94), with suggestive effect in incident CRC cases from population trials (CRC-specific survival, HR = 0.76; 95% CI: 0.39–1.13). No heterogeneity or publication bias was noted.
Conclusions
Meta-analysis demonstrates a clinically meaningful benefit of vitamin D supplementation on CRC survival outcomes. Further well-designed, adequately powered RCTs are needed to fully evaluate benefit of supplementation in augmenting ‘real-life’ follow-up and adjuvant chemotherapy regimens, as well as determining optimal dosing.
Background
Colorectal cancer (CRC) is the third most common cancer across the world, with 1.8 million cases and ~860,000 deaths each year.1 There is a 10-fold variation in incidence across the world with risk being highest in developed countries, suggesting that the disease may be largely preventable. Ecological variation in vitamin D levels between populations has been proposed as an environmental factor contributing to variation in CRC incidence.2
Controversy surrounds the role of vitamin D deficiency in the aetiology of several common cancers. The strongest available observational evidence supports a link between vitamin D and CRC.3,4,5 Numerous in vitro studies demonstrate vitamin D-induced growth arrest and apoptosis of CRC cells, modulation of the Wnt signalling pathway, DNA repair and immunomodulation,6 lending support to a causal relationship between vitamin D and cancer. However, observational data implicating vitamin D deficiency in CRC aetiology or survival are limited by potential bias: environmental risk factors associated with CRC are also associated with vitamin D status (co-causality; e.g. physical activity, obesity); heterogeneity in assay type and performance across studies; the development of CRC itself—or its treatment—may induce lower vitamin D levels (reverse causation).5 Mendelian randomisation is an approach that can provide evidence for causality, but studies have thus far failed to detect a causal association between blood 25-hydroxyvitamin D level and CRC risk.7 This may be due to weakness of the available genetic instruments, combined with powerful environmental influences, such as variation in exposure to vitamin D-making ultraviolet B (UVB) sunlight.
Large population trials to date, including the VITAL, VIDA and WHI trials, have shown that vitamin D supplementation did not provide any detectable difference in the incidence of CRC.8,9,10 Baron et al.11 also reported no reduction in risk of recurrent colorectal adenomas following 3–5 years of supplementation. However, several features of these studies may have limited the ability to detect any effect of supplementation on clinical endpoints.12,13 In brief, recruited subjects were predominantly already sufficient or replete for vitamin D, thereby blunting any health benefit that might be achieved; ‘off-protocol’ vitamin D supplementation was reported in control groups; population heterogeneity such as genetic (variable response or action of vitamin D due to participant genetics) and UVB exposure due to latitude of residence/outdoor activity was not considered as CRC incidence rate was low during follow-up.
In support of a causal effect, several studies have demonstrated an interaction between vitamin D-related genetic variation, 25-hydroxyvitamin D (25OHD) level and CRC or neoplasia risk or outcome, mitigating against potential confounding effects.14,15,16,17 In a sub-analysis of VITAL trial data, a lower rate of all cancer death was observed after 2 years of follow-up (hazard ratio (HR) = 0.75; 95% confidence interval (CI 0.59–0.96)). Furthermore, a recent meta-analysis found reduced total cancer mortality with vitamin D supplementation (HR = 0.87; 95% CI 0.79–0.96).18
Here, we present a systematic review and meta-analysis of randomised controlled trials examining the impact of vitamin D supplementation on progression and survival in patients with CRC.
Methods
Literature search
We performed two literature searches. First, to identify trials of vitamin D supplementation in CRC patients; second, to identify completed trials of vitamin D supplementation in non-cancer cohorts, which included cancer mortality as a trial outcome. The electronic databases PubMed19 and Web of Science20 were systematically searched for eligible trials from inception until 31 January 2020.
A comprehensive list of search terms directly relevant to the scope of this systematic review was created. For vitamin D, we included a wide range of terms, including vitamin D, 25-hydroxyvitamin D, calcidiol, cholecalciferol and 25OHD. For the intervention, the following terms were used: supplementation, intervention, treatment, placebo and RCT. For the patient population, we included terms: CRC, bowel, digestive, colon and rectum. Last, for the outcome we included terms: survival, prognosis, mortality and recurrence (Supplementary Table 1). For trials in non-cancer cohorts, the CRC terms were omitted (i.e. CRC, bowel, digestive, colon and rectum). We considered all human research original full-text articles with no restriction on follow-up duration or language, but excluded case reports, reviews and prior meta-analyses. The two searches returned 768 and 3333 articles, respectively. Bibliographies from obtained articles, relevant reviews and clinicaltrials.gov were searched with no further relevant and reported trials identified. To ensure all relevant trials had been included, we checked results against two recent meta-analyses of vitamin D supplementation and all cancer mortality,18,21 which did not yield any further trials. Titles/abstracts were screened by two researchers (P.G.V.-S. and L.F.B.), who then screened full texts for eligibility. The trial ‘PICO’ inclusion criteria were: (i) participants: individuals over the age of 18 years (with/without diagnosis of CRC); (ii) intervention: vitamin D supplementation; (iii) comparators: a placebo/lower dose of vitamin D; (iv) outcome: all measures of survival, for example, progression-free survival, overall survival (OS) and CRC-specific survival. Only randomised controlled trials were included. Disagreements at any stage were resolved by discussion with the senior author (M.G.D.). The review is registered on PROSPERO, registration number CRD42020173397.
Data extraction
Data extraction was conducted by two investigators (L.F.B. and P.G.V.-S.). The data from eligible trials were extracted into a prospectively designed database, including the following information: trial name, publication year, location, sample size, the trial duration, the active intervention (dose and frequency) and comparator (placebo or lower dose), treatment duration and total follow-up duration, the primary and secondary outcomes and the measured outcome (e.g. HR for OS, disease-free survival (DFS) or relapse-free survival and colorectal/disease-specific survival (DSS)). The most fully adjusted HR were extracted. Where the relevant HR were not reported, we contacted the trial authors by email to obtain these (N = 4 contacted, two authors provided relevant HR). For population trials, we included HR for CRC mortality from the time of randomisation in those trial subjects who developed CRC.
Quality assessment
An assessment of the methodological quality of the included trials was conducted using the 2010 CONSORT statement by two authors (L.F.B. and P.G.V.-S.) and disagreement resolved by discussion. Each trial was assessed for adherence against the CONSORT checklist as per previously reported methods.22,23,24 Adherence against 22 items was assessed and any trial with a high level of missing items (>50%) was considered at high risk of bias and excluded from quantitative assessment through meta-analysis.
Statistical analysis
The main analysis was a trial level meta-analysis of supplementation and CRC outcomes for all eligible trials. Secondary pre-specified sub-group meta-analyses were individually performed for colorectal-specific survival and DFS and for CRC and population trials. The extracted HRs and 95% CIs were used to calculate the pooled HR estimates. Standard errors were used to calculate weighting for each trial. The Hartung–Knapp–Sidik–Jonkman method was used to calculate pooled HR because of the a priori expected heterogeneity between trials, due to differences among populations and methodological dissimilarities between trials. This method was preferred over the DerSimonian and Laird random-effects model given the small number of trials included in the meta-analysis.25,26 The I2 statistic was calculated to quantify the degree of heterogeneity between trials and assess impact on the meta-analysis.27 Publication and selection bias was investigated by checking for asymmetry in the funnel plots and running the Egger’s regression test.28 All analyses were performed in R29 with the R-package ‘metafor’ used for meta-analyses.30
Results
Literature search
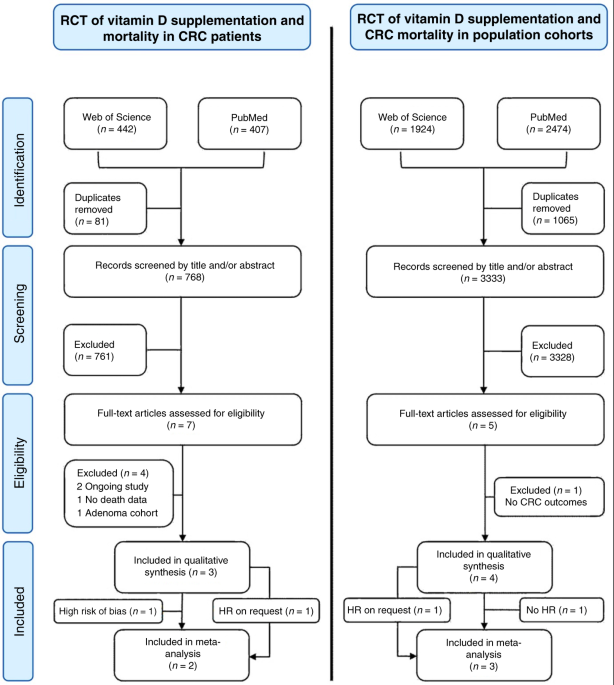
A flowchart illustrating trial selection process is shown in Fig. 1. After removal of duplicates, the two searches (in CRC patients and population trials) yielded 768 and 3333 trials, respectively. Full texts of seven trials in CRC patients and five population trials were considered for inclusion and assessed for eligibility. Full-text review and subsequent correspondence with trial authors yielded three relevant trials in CRC patients31,32,33 and four population trials for systematic review8,34,35 (Table 1).
Fig. 1: PRISMA flowchart of the trial selection process.
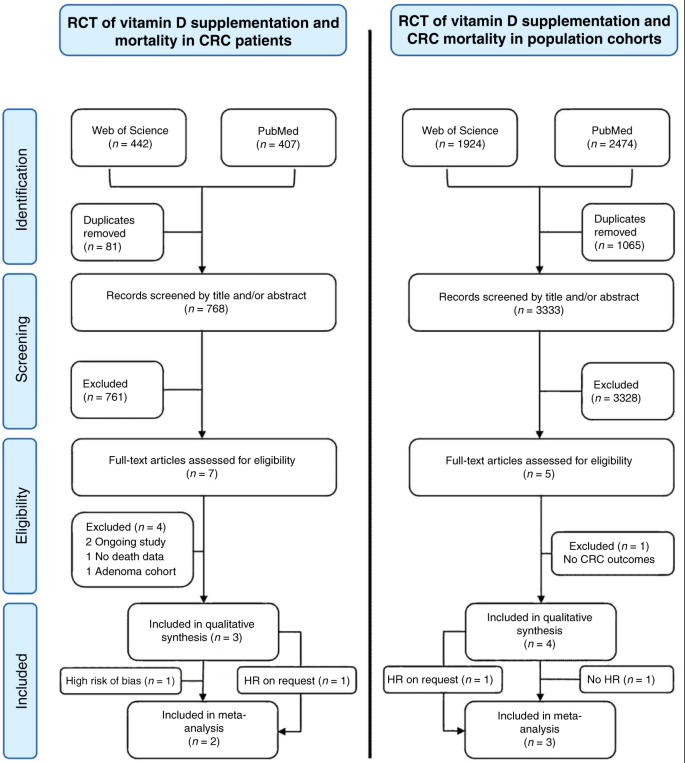
Excluded RCTs of supplementation in CRC patients were the D-health trial (ongoing trial,40) D2dca trial (not yet published); trials by Lappe et al.52 solely reported cancer incidence, but not survival outcomes; Baron et al.11 reported CRC incidence in an adenoma cohort, but with only 14 CRC cases.53 The excluded RCT of supplementation in population cohorts was the VIDA trial as CRC deaths were not reported or available on request;10 the RECORD trial reported CRC deaths,39 but a hazard ratio (HR) was not reported or available on request, so was excluded from meta-analysis. The Golubic et al.31 trial was not included in the meta-analysis of trials in CRC patients due to a high risk of bias, see below.
Full size image
Table 1 Characteristics of included trials.
Full size table
The main characteristics of included trials are summarised in Table 1. In brief, Golubic et al.31 found no effect of supplementation on OS in stage IV patients at 46 months (2000 IU/day; baseline median 25OHD 13.2 ng/ml, 70 (98.6%) of 71 patients insufficient (<20 ng/ml) at baseline, survival HR = 1.01; 95% CI: 0.39–2.61). In the SUNSHINE trial,32 70% (n = 87) patients had insufficient 25OHD at baseline, and 4000 IU/day supplementation increased median 25OHD from 16.1 to 34.8 ng/ml (87 (70%) with improved median progression-free survival from 11.0 to 13.0 months in stage IV CRC patients (HR = 0.64; 95% CI: 0–0.90; median follow-up 23 months). In the AMATERASU trial,33 41% (n = 173) patients had insufficient 25OHD at baseline, with 2000 IU/day supplementation associated with a non-significant improvement in survival with supplementation after median follow-up 3.5 years in stage I–III patients (25OHD ~20 ng/ml at baseline, ~60 ng/ml at follow-up; HR = 0.69; 95% CI: 0.39–1.24). In the population trials, 400 IU/day in the Women’s Health Initiative trial8 did not impact CRC mortality (baseline median 25OHD 18.4 ng/ml; proportion of insufficient participants at baseline not given; HR = 0.82; 95% CI: 0.52–1.29), with similar results reported by Trivedi et al.34 (100,000 IU/4-monthly; proportion of insufficient participants at baseline not given; follow-up 25OHD 29.7 vs. 21.4 ng/ml with placebo; HR = 0.62; 95% CI: 0.24–1.60). The VITAL trial35 authors provided relevant data on request, with a trend towards increased DSS and PFS in 98 incident CRC cases (only 2001 (13%) insufficient for 25OHD at baseline; 25OHD 29.8 ng/ml to 41.8 ng/ml in treatment arm; DSS HR = 0.65; 95% CI: 0.28–1.50); PFS HR = 0.79; 95% CI: 0.36–1.75). In the RECORD trial36 of secondary fracture prevention, there was no impact on CRC death in 71 incident CRC cases, with 20 CRC deaths in the vitamin D group and 13 in the placebo/calcium groups (baseline 25OHD 15.2 ng/ml; HR not available on request).
Quality assessment
Adherence to the CONSORT 2010 checklist37 was assessed for the seven trials identified in the literature search, with high rates of adherence for all but the Golubic trial (Supplementary Table 2). In particular, it was noted that this trial was not placebo controlled, with no reported mechanism to implement the random allocation sequence, no eligibility criteria for participants given and no description of level and method of blinding given. As a result, this trial was considered at high risk of bias and excluded from overall meta-analysis.
Meta-analysis of vitamin D supplementation and survival outcomes
All included trials demonstrated a beneficial effect. Overall meta-analysis in five trials, comprising 815 participants revealed a beneficial effect of vitamin D supplementation on cancer outcomes in patients with CRC (HR = 0.70; 95% CI: 0.48–0.93; Fig. 2). Sub-group meta-analyses demonstrated a consistent favourable effect with vitamin D supplementation. In trials recruiting patients with CRC at outset, CRC progression or death was reduced by 35% (HR = 0.65; 95% CI:0.36–0.94; Fig. 3a), and by 33% across the three trials reporting PFS (HR = 0.67; 95% CI: 0.40–0.94; Fig. 3b). In the population trials, disease-specific survival improved by 24% (HR = 0.76; 95% CI: 0.39–1.13; Fig. 3c). Results were not quantitatively changed when the excluded Golubic et al.31 trial was included in the meta-analysis (Supplementary Fig. 1).
Fig. 2: Meta-analysis of the effect of vitamin D supplementation on CRC outcomes.
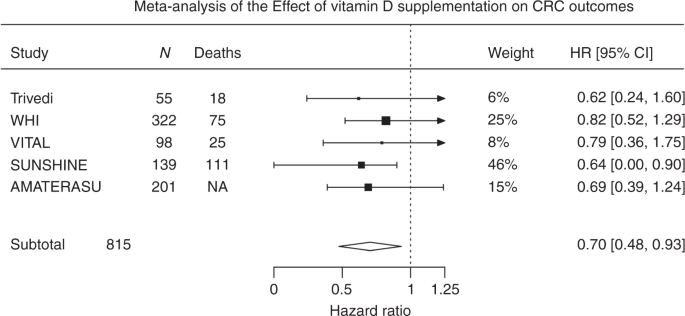
HRs used are for disease (CRC)-specific survival for the Trivedi and Women’s Health initiative (WHI) trials and progression-free survival for the VITAL, SUNSHINE and AMATERASU trials. HR confidence interval in the SUNSINE trial was one-sided. There was no evidence of heterogeneity with τ: 0.026; I2 (total heterogeneity/total variability): 0.85% and P = 0.98.
Full size image
Fig. 3: Sub-group meta-analyses results.
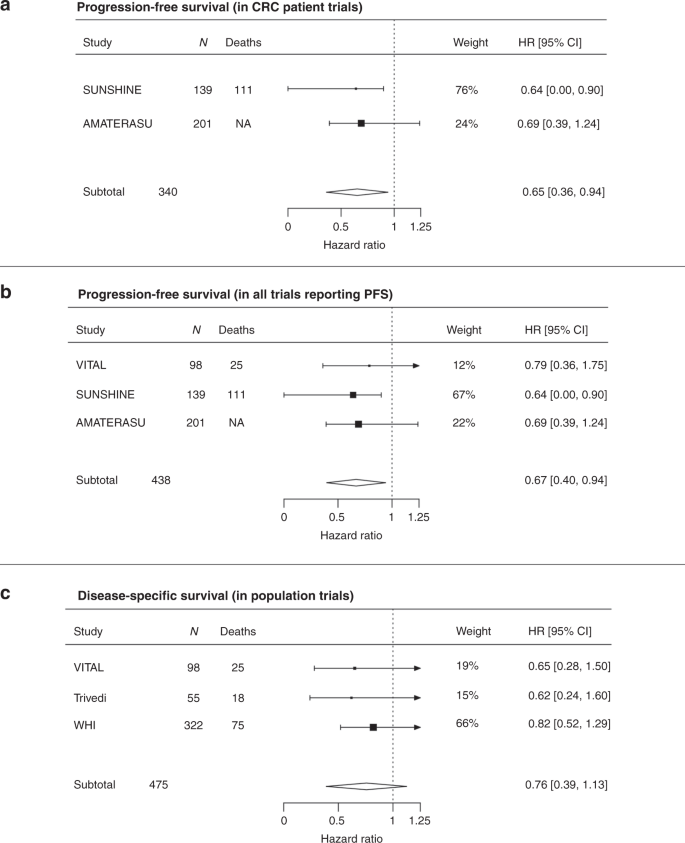
HRs used are for disease (CRC) specific survival for the Trivedi and Women’s Health initiative (WHI) trials and progression-free survival for the VITAL, SUNSHINE and AMATERASU trials. Statistical testing in the SUNSINE trial was one-sided. There was no evidence of heterogeneity in sub-group meta-analyses presented in a–c with τ < 0.03; I2 (total heterogeneity/total variability): <0.6% and P > 0.88.
Full size image
Testing for trial heterogeneity and publication bias
Despite the different interventions and outcomes in the included trials, there was no evidence of heterogeneity with τ: 0.026 and I2: 0.85% in the overall meta-analysis. No evidence of publication bias was seen, with Egger’s regression test for funnel plot asymmetry P = 0.87 (Supplementary Fig. 2).38
Discussion
This is the first systematic review with meta-analysis of randomised controlled trials to examine the effect of vitamin D supplementation on survival outcomes in patients with CRC. We found that supplementation imparts a 30% reduction in adverse survival outcomes overall, with a 24% reduction in CRC-specific death and a 33% in disease progression or death. The effect on survival was consistently observed in sub-group analyses both in trials specifically including CRC patients and in population trials reporting outcomes in incident CRC cases.
We included two RCTs of supplementation in patients with a diagnosis of CRC and demonstrated a 35% reduction in CRC progression or death with supplementation. We also recognised that incident cases of CRC occur in large population trials, providing an additional source of trial evidence. We included three population trials totalling almost 65,000 participants in our meta-analysis, with a suggestive benefit from supplementation on CRC-specific survival (HR = 0.76; 95% CI: 0.39–1.12). Two relevant trials were not included as HRs for CRC outcomes were not available after requests to the author,10,39 while we identified several ongoing trials yet to publish results, or example, the D-Health trial.40
The VITAL trial authors recently performed a review and meta-analysis of supplementation and all cancer mortality based on incident cancers in population supplementation trials,18,35 reporting a reduction in total cancer mortality with supplementation (HR = 0.83; 95% CI: 0.67–1.02). A similar meta-analysis by Zhang et al.21 found a similar effect (HR = 0.84; 95% CI: 0.74–0.95), yet combining all cancers may be flawed given that ‘cancer’ is a not a single disease, but a hugely heterogeneous group of individual and specific diseases. The current literature review is the first to assimilate evidence from trials specifically including patients with a diagnosis of CRC, but also large population trials that reported survival outcomes in incident CRC cases. A consistent reduction in adverse survival outcomes irrespective of the trial inclusion criteria, supplementation dose or survival outcome measure is supportive of a true causal effect, which supports observational data linking 25OHD level and cancer outcomes.16,17
There are a number of limitations in the currently available trial data impacting on this analysis. First, our literature search demonstrates a lack of well-designed and adequately powered randomised controlled trials investigating vitamin D supplementation and CRC outcomes. All included trials in the current meta-analysis were small, each including <500 CRC cases amounting to only 815 cases in meta-analysis. Next, the population trials included here did not report any data on stage, site or subtype of incident CRC cases or adjuvant therapy used, which are known to impact survival outcomes and the variables used for the HR adjustment are not consistently reported. Third, observational data strongly supports an association between genetic factors related to vitamin D metabolism or function and survival outcomes,14,16,17 yet no trial to date has considered the relevance of genetic heterogeneity to the impact of vitamin D on cancer death. Finally, we acknowledge that pooling estimates from trials with differing methodology may limit the conclusions that can be drawn. For example, in the population trials, the two groups are comparable at point of randomisation, but may not be comparable at point of diagnosis of CRC, which could bias outcomes. However, variability in inclusion criteria, interventions or outcomes generally results in a more heterogeneous estimate and is likely to increase statistical uncertainty and hence results tend towards the null. Nonetheless, our summary findings (i.e. direction and magnitude of effect size) remain largely unchanged when the analysis was limited according to trial methodology or outcome.
We acknowledge that translation of results from supplement RCTs to a real-life healthcare setting is not always straight forward. While vitamin D is cheap and generally safe, vitamin D intoxication or other adverse effects of supplementation must be considered. Poor compliance may also impact on real-life benefit. Lower 25OHD level is strongly associated with CRC survival in observational data,14,16,17 providing a strong rationale for supplementation trials in cancer patients with survival outcomes as the defined endpoint yet observational studies of vitamin D supplementation or intake and survival do not provide consistent evidence of benefit from vitamin D. A Norwegian study recently reported better CRC survival in incident CRC cases with pre-diagnostic vitamin D intake of >400 IU/day (HR = 0.75; 95% CI: 0.61–0.92).41 Similarly, the Cancer Prevention Study-II reported a trend towards greater OS in those with higher total or dietary vitamin D intake (HR = 0.88; 95% CI: 0.57–1.35 and HR = 0.90; 95% CI: 0.67–1.21), yet even in quartile four, the intake was low (~>245 IU/day).42 Jeffreys et al.43 reported a non-significant reduction in mortality after CRC diagnosis in women who had been prescribed vitamin D supplementation in the 5 years preceding CRC diagnosis (13% of 4122 cases prescribed supplements; HR = 0.90; 95% CI: 0.78–1.04), yet some other studies have found no benefit from low-dose supplementation.44,45,46 Crucially, all of these studies assess low doses of supplementation or intake and do not consider vitamin D-related genetic variants that have been shown to influence the association between vitamin D and survival.14,16,17 The lack of consistent findings in the observational data support further well-powered trials investigating the role of appropriate supplementary doses of vital D in CRC patients with insufficient 25OHD levels at baseline. The above findings, together with the clear benefit of 4000 IU over 400 IU in the SUNSHINE study, suggest that an intake of 400 IU/day is inadequate. Indeed, it is noted that the reference nutrient intake for vitamin D of 400 IU/day is recommended for the UK population, with this intake given as the average amount needed by 97.5% of the population to maintain a serum 25OHD concentration ≥10 ng/l when UVB sunshine exposure is minimal.5 The optimal dose for survival benefit remains unclear and requires further investigation, but given that data from several publications and national bodies indicates 2000–4000 IU/day to be safe,5,47,48,49,50,51 we believe that doses of ~2000–4000 IU should be considered for future trials.
In conclusion, this meta-analysis demonstrates a clinically meaningful beneficial effect from vitamin D supplementation on survival outcomes in patients with CRC. Further well-designed, adequately powered RCTs are needed to fully evaluate the benefit of supplementation in augmenting ‘real-world’ follow-up and adjuvant chemotherapy regimens, as well as determining optimal dosing.
References
1.
Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A. & Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 68, 394–424 (2018).
Google Scholar
2.
Giovannucci, E. The epidemiology of vitamin D and cancer incidence and mortality: a review (United States). Cancer Causes Control 16, 83–95 (2005).
PubMed Google Scholar
3.
Theodoratou, E., Tzoulaki, I., Zgaga, L. & Ioannidis, J. P. Vitamin D and multiple health outcomes: umbrella review of systematic reviews and meta-analyses of observational studies and randomised trials. BMJ 348, g2035 (2014).
PubMed PubMed Central Google Scholar
4.
Autier, P., Boniol, M., Pizot, C. & Mullie, P. Vitamin D status and ill health: a systematic review. Lancet Diabetes Endocrinol. 2, 76–89 (2014).
CAS PubMed Google Scholar
5.
SACN. Vitamin D and Health (Scientific Advisory Committee on Nutrition, 2016).
6.
Fleet, J. C., DeSmet, M., Johnson, R. & Li, Y. Vitamin D and cancer: a review of molecular mechanisms. Biochem. J. 441, 61–76 (2012).
CAS PubMed PubMed Central Google Scholar
7.
He, Y., Timofeeva, M., Farrington, S. M., Vaughan-Shaw, P., Svinti, V., Walker, M. et al. Exploring causality in the association between circulating 25-hydroxyvitamin D and colorectal cancer risk: a large Mendelian randomisation study. BMC Med. 16, 142 (2018).
PubMed PubMed Central Google Scholar
8.
Wactawski-Wende, J., Kotchen, J. M., Anderson, G. L., Assaf, A. R., Brunner, R. L., O’Sullivan, M. J. et al. Calcium plus vitamin D supplementation and the risk of colorectal cancer. N. Engl. J. Med. 354, 684–696 (2006).
CAS PubMed Google Scholar
9.
Manson, J. E., Cook, N. R., Lee, I. M., Christen, W., Bassuk, S. S., Mora, S. et al. Vitamin D supplements and prevention of cancer and cardiovascular disease. N. Engl. J. Med. 380, 33–44 (2019).
CAS PubMed Google Scholar
10.
Scragg, R. K. R. Overview of results from the Vitamin D Assessment (ViDA) study. J. Endocrinol. Invest. 42, 1391–1399 (2019).
CAS PubMed Google Scholar
11.
Baron, J. A., Barry, E. L., Mott, L. A., Rees, J. R., Sandler, R. S., Snover, D. C. et al. A trial of calcium and vitamin D for the prevention of colorectal adenomas. N. Engl. J. Med. 373, 1519–1530 (2015).
CAS PubMed PubMed Central Google Scholar
12.
Vaughan-Shaw, P. G., Zgaga, L., Theodoratou, E., Blackmur, J. P. & Dunlop, M. G. Whether vitamin D supplementation protects against colorectal cancer risk remains an open question. Eur. J. Cancer 115, 1–3 (2019).
CAS PubMed Google Scholar
13.
Lappe, J. M. & Heaney, R. P. Why randomized controlled trials of calcium and vitamin D sometimes fail. Dermatoendocrinology 4, 95–100 (2012).
CAS Google Scholar
14.
Zgaga, L., Theodoratou, E., Farrington, S. M., Din, F. V., Ooi, L. Y., Glodzik, D. et al. Plasma vitamin D concentration influences survival outcome after a diagnosis of colorectal cancer. J. Clin. Oncol. 32, 2430–2439 (2014).
CAS PubMed Google Scholar
15.
Barry, E. L., Peacock, J. L., Rees, J. R., Bostick, R. M., Robertson, D. J., Bresalier, R. S. et al. Vitamin D receptor genotype, vitamin D3 supplementation, and risk of colorectal adenomas: a randomized clinical trial. JAMA Oncol. https://doi.org/10.1001/jamaoncol.2016.5917 (2016).
16.
Vaughan-Shaw, P. G., Zgaga, L., Ooi, L. Y., Theodoratou, E., Timofeeva, M., Svinti, V. et al. Low plasma vitamin D is associated with adverse colorectal cancer survival after surgical resection, independent of systemic inflammatory response. Gut 69, 103–111 (2020)
17.
Vaughan-Shaw, P. G., O’Sullivan, F., Farrington, S. M., Theodoratou, E., Campbell, H., Dunlop, M. G. et al. The impact of vitamin D pathway genetic variation and circulating 25-hydroxyvitamin D on cancer outcome: systematic review and meta-analysis. Br. J. Cancer 116, 1092–1110 (2017).
CAS PubMed PubMed Central Google Scholar
18.
Keum, N., Lee, D. H., Greenwood, D. C., Manson, J. E. & Giovannucci, E. Vitamin D supplementation and total cancer incidence and mortality: a meta-analysis of randomized controlled trials. Ann. Oncol. 30, 733–743 (2019).
CAS PubMed PubMed Central Google Scholar
19.
NCBI. PubMed http://www.ncbi.nlm.nih.gov/pubmed/advanced (2015).
20.
JISC. Web of Science http://wok.mimas.ac.uk/ (2015).
21.
Zhang, Y., Fang, F., Tang, J. J., Jia, L., Feng, Y. N., Xu, P. et al. Association between vitamin D supplementation and mortality: systematic review and meta-analysis. BMJ 366, https://doi.org/10.1136/bmj.l4673 (2019).
22.
McCormick, F., Cvetanovich, G. L., Kim, J. M., Harris, J. D., Gupta, A. K., Abrams, G. D. et al. An assessment of the quality of rotator cuff randomized controlled trials: utilizing the Jadad score and CONSORT criteria. J. Shoulder Elb. Surg. 22, 1180–1185 (2013).
Google Scholar
23.
Moher, D., Jones, A., Lepage, L. & Group, C. Use of the CONSORT statement and quality of reports of randomized trials: a comparative before-and-after evaluation. JAMA 285, 1992–1995 (2001).
CAS PubMed Google Scholar
24.
Sut, N., Senocak, M., Uysal, O. & Koksalan, H. Assessing the quality of randomized controlled trials from two leading cancer journals using the CONSORT statement. Hematol. Oncol. Stem Cell Ther. 1, 38–43 (2008).
PubMed Google Scholar
25.
Cornell, J. E., Mulrow, C. D., Localio, R., Stack, C. B., Meibohm, A. R., Guallar, E. et al. Random-effects meta-analysis of inconsistent effects: a time for change. Ann. Intern. Med. 160, 267–270 (2014).
PubMed Google Scholar
26.
IntHout, J., Ioannidis, J. P. & Borm, G. F. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med. Res. Methodol. 14, 25 (2014).
PubMed PubMed Central Google Scholar
27.
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ 327, 557–560 (2003).
PubMed PubMed Central Google Scholar
28.
Sterne, J. A. & Egger, M. Funnel plots for detecting bias in meta-analysis: guidelines on choice of axis. J. Clin. Epidemiol. 54, 1046–1055 (2001).
CAS PubMed Google Scholar
29.
R Foundation for Statistical Computing. R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, Vienna, Austria, 2013).
30.
Viechtbauer, W. & Cheung, M. W. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 1, 112–125 (2010).
PubMed Google Scholar
31.
Antunac Golubic, Z., Barsic, I., Librenjak, N. & Plestina, S. Vitamin D supplementation and survival in metastatic colorectal cancer. Nutr. Cancer 70, 413–417 (2018).
CAS PubMed Google Scholar
32.
Ng, K., Nimeiri, H. S., McCleary, N. J., Abrams, T. A., Yurgelun, M. B., Cleary, J. M. et al. Effect of high-dose vs standard-dose vitamin D3 supplementation on progression-free survival among patients with advanced or metastatic colorectal cancer: the SUNSHINE randomized clinical trial. JAMA 321, 1370–1379 (2019).
CAS PubMed PubMed Central Google Scholar
33.
Urashima, M., Ohdaira, H., Akutsu, T., Okada, S., Yoshida, M., Kitajima, M. et al. Effect of vitamin D supplementation on relapse-free survival among patients with digestive tract cancers: the AMATERASU randomized clinical trial. JAMA 321, 1361–1369 (2019).
CAS PubMed PubMed Central Google Scholar
34.
Trivedi, D. P., Doll, R. & Khaw, K. T. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomised double blind controlled trial. BMJ 326, 469 (2003).
CAS PubMed PubMed Central Google Scholar
35.
Manson, J. E., Bassuk, S. S., Buring, J. E. & Group, V. R. Principal results of the VITamin D and OmegA-3 TriaL (VITAL) and updated meta-analyses of relevant vitamin D trials. J. Steroid Biochem. Mol. Biol. 198, 105522 (2019).
PubMed Google Scholar
36.
Avenell, A., MacLennan, G. S., Jenkinson, D. J., McPherson, G. C., McDonald, A. M., Pant, P. R. et al. Long-term follow-up for mortality and cancer in a randomized placebo-controlled trial of vitamin D(3) and/or calcium (RECORD trial). J. Clin. Endocrinol. Metab. 97, 614–622 (2012).
CAS PubMed Google Scholar
37.
Schulz, K. F., Altman, D. G., Moher, D. & Group, C. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 340, c332 (2010).
PubMed PubMed Central Google Scholar
38.
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634 (1997).
CAS PubMed PubMed Central Google Scholar
39.
Avenell, A., MacLennan, G. S., Jenkinson, D. J., McPherson, G. C., McDonald, A. M., Pant, P. R. et al. Long-term follow-up for mortality and cancer in a randomized placebo-controlled trial of vitamin D-3 and/or calcium (RECORD Trial). J. Clin. Endocrinol. Metab. 97, 614–622 (2012).
CAS PubMed Google Scholar
40.
Neale, R. E., Armstrong, B. K., Baxter, C., Duarte Romero, B., Ebeling, P., English, D. R. et al. The D-Health trial: a randomized trial of vitamin D for prevention of mortality and cancer. Contemp. Clin. Trials 48, 83–90 (2016).
CAS PubMed Google Scholar
41.
Oyeyemi, S. O., Braaten, T., Skeie, G. & Borch, K. B. Competing mortality risks analysis of prediagnostic lifestyle and dietary factors in colorectal cancer survival: the Norwegian Women and Cancer Study. BMJ Open Gastroenterol. 6, e000338 (2019).
PubMed PubMed Central Google Scholar
42.
Yang, B., McCullough, M. L., Gapstur, S. M., Jacobs, E. J., Bostick, R. M., Fedirko, V. et al. Calcium, vitamin D, dairy products, and mortality among colorectal cancer survivors: the Cancer Prevention Study-II Nutrition Cohort. J. Clin. Oncol. 32, 2335–2343 (2014).
CAS PubMed Google Scholar
43.
Jeffreys, M., Redaniel, M. T. & Martin, R. M. The effect of pre-diagnostic vitamin D supplementation on cancer survival in women: a cohort study within the UK Clinical Practice Research Datalink. BMC Cancer 15, 670 (2015).
PubMed PubMed Central Google Scholar
44.
Lewis, C., Xun, P. & He, K. Vitamin D supplementation and quality of life following diagnosis in stage II colorectal cancer patients: a 24-month prospective study. Support Care Cancer 24, 1655–1661 (2016).
PubMed Google Scholar
45.
Inoue-Choi, M., Greenlee, H., Oppeneer, S. J. & Robien, K. The association between postdiagnosis dietary supplement use and total mortality differs by diet quality among older female cancer survivors. Cancer Epidemiol. Biomark. Prev. 23, 865–875 (2014).
CAS Google Scholar
46.
Ng, K., Meyerhardt, J. A., Chan, J. A., Niedzwiecki, D., Hollis, D. R., Saltz, L. B. et al. Multivitamin use is not associated with cancer recurrence or survival in patients with stage III colon cancer: findings from CALGB 89803. J. Clin. Oncol. 28, 4354–4363 (2010).
PubMed PubMed Central Google Scholar
47.
Hathcock, J. N., Shao, A., Vieth, R. & Heaney, R. Risk assessment for vitamin D. Am. J. Clin. Nutr. 85, 6–18 (2007).
CAS PubMed Google Scholar
48.
Stamp, T. C., Haddad, J. G. & Twigg, C. A. Comparison of oral 25-hydroxycholecalciferol, vitamin D, and ultraviolet light as determinants of circulating 25-hydroxyvitamin D. Lancet 1, 1341–1343 (1977).
CAS PubMed Google Scholar
49.
Jones, G. Pharmacokinetics of vitamin D toxicity. Am. J. Clin. Nutr. 88, 582S–586S (2008).
CAS PubMed Google Scholar
50.
Vieth, R. Vitamin D toxicity, policy, and science. J. Bone Miner. Res 22(Suppl. 2), V64–V68 (2007).
CAS PubMed Google Scholar
51.
Azzi, A., Brigelius-Flohe, R., Kelly, F., Lodge, J. K., Ozer, N., Packer, L. et al. On the opinion of the European Commission “Scientific Committee on Food” regarding the tolerable upper intake level of vitamin E (2003). Eur. J. Nutr. 44, 60–62 (2005).
PubMed Google Scholar
52.
Lappe, J. M., Travers-Gustafson, D., Davies, K. M., Recker, R. R. & Heaney, R. P. Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am. J. Clin. Nutr. 85, 1586–1591 (2007).
CAS PubMed Google Scholar
53.
Calderwood, A. H., Baron, J. A., Mott, L. A., Ahnen, D. J., Bostick, R. M., Figueiredo, J. C. et al. No evidence for posttreatment effects of vitamin D and calcium supplementation on risk of colorectal adenomas in a randomized trial. Cancer Prev. Res. (Philos.) 12, 295–304 (2019).
CAS Google Scholar
Download references
Author information
Author notes
These authors contributed equally: Peter G. Vaughan-Shaw, Louis F. Buijs, Susan M. Farrington, Malcolm G. Dunlop
Affiliations
MRC Human Genetics Unit, Institute of Genetics and Molecular Medicine, University of Edinburgh, Edinburgh, UK
Peter G. Vaughan-Shaw, Louis F. Buijs, James P. Blackmur, Farhat V. N. Din, Susan M. Farrington & Malcolm G. Dunlop
Cancer Research UK Edinburgh Centre, Institute of Genetics and Molecular Medicine, University of Edinburgh, Edinburgh, UK
Peter G. Vaughan-Shaw, Louis F. Buijs, James P. Blackmur, Evi Theodoratou, Farhat V. N. Din, Susan M. Farrington & Malcolm G. Dunlop
Centre for Global Health Research, Usher Institute for Population Health Sciences and Informatics, University of Edinburgh, Edinburgh, UK
Evi Theodoratou
Department of Public Health and Primary Care, Trinity College Dublin, Dublin, Ireland
Lina Zgaga
Contributions
P.G.V.-S.: conceptualisation, methodology, formal analysis, writing—original draft, visualisation, writing—review and editing. L.F.B.: methodology, formal analysis, writing—original draft. J.P.B.: conceptualisation, writing—review and editing. E.T.—methodology, writing—review and editing. L.Z.: conceptualisation, methodology, writing—review and editing. F.V.N.D.: conceptualisation, methodology, writing—review and editing. S.M.F.: supervision, writing—review and editing. M.G.D.: conceptualisation, project administration, funding acquisition, supervision, writing—review and editing.
Corresponding author
Correspondence to Malcolm G. Dunlop.
Ethics declarations
Ethics approval and consent to participate
Not required; data were collected for previously published studies.
Data availability
Available at reasonable requests from pvaughan@ed.ac.uk.
Competing interests
The authors declare no competing interests
Funding information
This work was supported by funding for the infrastructure and staffing of the Edinburgh CRUK Cancer Research Centre; CRUK programme grant C348/A18927 (M.G.D.). P.G.V.-S. was supported by a NES SCREDS clinical lectureship. J.P.B. is supported by an ECAT-linked CRUK ECRC Clinical training award (C157/A23218). E.T. is supported by a CRUK Career Development Fellowship (C31250/A22804). F.V.N.D. is supported by a CSO Senior Clinical Fellowship. This work was also funded by a grant to M.G.D. as Project Leader with the MRC Human Genetics Unit Centre Grant (U127527202 and U127527198 from 1/4/18).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information
Cytotoxic CD8+ T cells in cancer and cancer immunotherapy
Cytotoxic CD8<sup>+</sup> T cells in cancer and cancer immunotherapy:
British Journal of Cancer, Published online: 15 September 2020; doi:10.1038/s41416-020-01048-4
Cytotoxic CD8+ T cells in cancer and cancer immunotherapy
Abstract
The functions of, and interactions between, the innate and adaptive immune systems are vital for anticancer immunity. Cytotoxic T cells expressing cell-surface CD8 are the most powerful effectors in the anticancer immune response and form the backbone of current successful cancer immunotherapies. Immune-checkpoint inhibitors are designed to target immune-inhibitory receptors that function to regulate the immune response, whereas adoptive cell-transfer therapies use CD8+ T cells with genetically modified receptors—chimaeric antigen receptors—to specify and enhance CD8+ T-cell functionality. New generations of cytotoxic T cells with genetically modified or synthetic receptors are being developed and evaluated in clinical trials. Furthermore, combinatory regimens might optimise treatment effects and reduce adverse events. This review summarises advances in research on the most prominent immune effectors in cancer and cancer immunotherapy, cytotoxic T cells, and discusses possible implications for future cancer treatment.
British Journal of Cancer, Published online: 15 September 2020; doi:10.1038/s41416-020-01048-4
Cytotoxic CD8+ T cells in cancer and cancer immunotherapy
Abstract
The functions of, and interactions between, the innate and adaptive immune systems are vital for anticancer immunity. Cytotoxic T cells expressing cell-surface CD8 are the most powerful effectors in the anticancer immune response and form the backbone of current successful cancer immunotherapies. Immune-checkpoint inhibitors are designed to target immune-inhibitory receptors that function to regulate the immune response, whereas adoptive cell-transfer therapies use CD8+ T cells with genetically modified receptors—chimaeric antigen receptors—to specify and enhance CD8+ T-cell functionality. New generations of cytotoxic T cells with genetically modified or synthetic receptors are being developed and evaluated in clinical trials. Furthermore, combinatory regimens might optimise treatment effects and reduce adverse events. This review summarises advances in research on the most prominent immune effectors in cancer and cancer immunotherapy, cytotoxic T cells, and discusses possible implications for future cancer treatment.
Εγγραφή σε:
Σχόλια (Atom)